Bell’s Palsy: What It Is, What to Expect, and When to Act Fast
Posted by Dr Akhilesh Kumar | Paralysis Treatment in Lucknow
What Is Bell’s Palsy (Facial Paralysis) — In Simple Words?
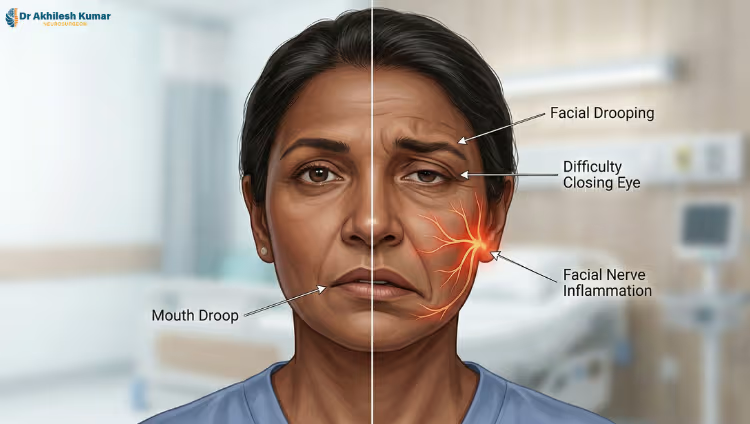
One morning, you wake up, and one side of your face is not moving. Your mouth droops. Your eye won’t close. You can’t smile properly. It feels terrifying — and your first thought is stroke.
Bell’s palsy is not a stroke. It is a sudden weakness or paralysis of the facial nerve — the nerve that controls movement on one side of your face. When this nerve gets inflamed and swollen, it gets compressed inside a very narrow bony canal in your skull. There is no space for the swelling to escape. Pressure builds, blood supply drops, and the nerve stops working properly.
The facial nerve does much more than move your face. It controls your ability to close your eyes, taste food, produce tears, control saliva, and even reduce loud sounds. So when it is damaged, the effects go far beyond a drooping face.
The good news is that most people recover. But how well — and how fully — depends almost entirely on what happens in the first few days.
Bell’s Palsy vs Stroke — The Difference You Must Know
This is the most important question in the first hour. Both can cause facial drooping. But they are very different conditions requiring very different treatment.
The single most important test you can do at home: Ask the person to raise their eyebrows.
If the forehead and eyebrows move normally but the lower face droops — this points toward a stroke. The upper face is controlled differently in the brain and is often spared in strokes.
If the entire side of the face is weak — forehead, eye, and mouth together — this is more likely Bell’s palsy, which is a peripheral nerve problem.
However, do not guess. Brainstem strokes can sometimes look exactly like Bell’s palsy. If there is any headache, dizziness, imbalance, double vision, or confusion alongside facial weakness, go to the emergency department immediately. When in doubt, a scan is always safer than a wait-and-see approach.
What Causes Bell’s Palsy?
The most common explanation is a viral infection — particularly the reactivation of the Herpes Simplex Virus (the same virus that causes cold sores). The virus inflames the facial nerve inside its bony canal.
But that is not the only cause. Other triggers include:
- Diabetes affects the tiny blood vessels supplying the nerve
- Pregnancy, especially in the third trimester
- Post-viral immune reactions
- Lyme disease in certain regions
- Sarcoidosis or other inflammatory conditions
- In rare cases, a tumour presses on the nerve
When doctors say the cause is “idiopathic,” it simply means the exact trigger was not found. That matters — because if Bell’s palsy does not improve as expected, those other causes must be investigated.
What Actually Determines How Well You Recover?
Recovery from Bell’s palsy is not about hope or willpower. It is about nerve biology. Three things decide your outcome:
Bell’s Palsy Recovery: What Shapes Your Outcome
| Factor | Best Case | Worst Case |
|---|---|---|
| Type of nerve damage | Only the protective coating is damaged (demyelination) — nerve signal returns fast | The nerve fibre itself is damaged (axonal degeneration) — recovery takes months and may be incomplete |
| When steroids are started | Within 72 hours — strong evidence of better recovery | After 7 days — benefit drops sharply |
| Eye protection | Artificial tears used regularly, eye taped at night — cornea stays safe | Eye left unprotected — permanent vision damage can occur |
| Facial exercises | Done correctly under guidance — helps recovery | Done aggressively without guidance — can cause permanent tightness and miswiring |
| Follow-up care | Regular check-ins, synkinesis caught early | No follow-up — complications develop silently |
The first 72 hours after Bell’s palsy begins are the most critical window in the entire recovery journey.
Step-by-Step: What Treatment Looks Like
Steroids — the most important medicine, Prednisolone (a steroid) given within 72 hours of symptoms starting is the most evidence-backed treatment available. It reduces swelling around the nerve and significantly improves chances of full recovery. After one week, the benefit drops sharply. After three weeks, it is unlikely to help at all.
Antiviral medicines, Antivirals like acyclovir, are sometimes added, especially in severe cases. The evidence is less clear, but many specialists include them given the suspected viral cause.
Eye protection — non-negotiable Because the eye cannot close properly, the cornea dries out. This can cause serious and permanent eye damage. Artificial tears must be used regularly throughout the day. At night, the eye must be taped shut or covered. This is not optional. Many patients focus so much on their face that they neglect their eye — and that is where lasting damage quietly occurs.
Physiotherapy — helpful but must be guided, Gentle, specific facial exercises under the guidance of a trained therapist help the nerve recover correctly. However, aggressive, unstructured exercises done too early or too intensely can wire the nerve incorrectly — causing a complication called synkinesis (explained below).
The Complication Nobody Warns You About: Synkinesis
This is what happens to many patients who appear to have “recovered” — but feel something is still wrong.
Synkinesis means the nerve grew back incorrectly. As they regrow, nerve fibres take the wrong paths and connect to the wrong muscles. The result is involuntary, linked movements — movements you did not choose to make.
Common examples include: your eye closing when you smile, your mouth twitching when you blink, and your face feeling constantly tight even at rest. It is not rare. It is simply underreported because most basic guides never mention it.
Synkinesis can be managed with targeted neuromuscular retraining by a specialist physiotherapist, and sometimes with carefully placed Botulinum toxin (Botox) injections to relax overactive muscles. But the most important point is this: aggressive facial exercises in the early stages can increase the risk of synkinesis. This is why doing exercises from a random internet video without professional guidance is genuinely risky.
When Bell’s Palsy Is NOT What It Seems
Most facial nerve problems are straightforward Bell’s palsy. But certain signs must not be ignored, because they point to something more serious requiring urgent investigation:
- Weakness that gradually gets worse over several weeks
- Facial weakness that comes back on the same side after recovering
- Both sides of the face are affected
- True numbness on the face — not just weakness
- Severe pain that seems out of proportion
- Hearing loss alongside facial weakness
- Other neurological symptoms were present at the same time
In these cases, an MRI with contrast of the facial nerve canal is not over-testing — it is essential. Missing a tumour of the facial nerve or the parotid gland because imaging was skipped is a serious and avoidable outcome.
Bell’s Palsy During Pregnancy
Bell’s palsy occurs more frequently in the third trimester of pregnancy. The reasons include fluid retention putting pressure on the nerve, changes in the immune system, and altered blood flow. Steroid treatment is still generally used but requires a careful discussion between the patient, her obstetrician, and her neurologist regarding timing, dosage, and risk to the baby. This situation should never be managed with general advice from the internet.
When to Go Back to Your Doctor Immediately
Do not wait if any of the following occur:
- Weakness is still getting worse after three weeks
- No improvement at all by three months
- Severe or worsening pain
- The same side is affected again
- Both sides of the face become affected
- Any new neurological symptom appears
At this point, what started as Bell’s palsy becomes a diagnostic investigation. Further testing and specialist review are not optional.
Frequently Asked Questions About Bell’s Palsy
Q1. Is Bell’s palsy permanent?
In most cases, no. Around 70 to 85 percent of patients recover fully within three to six months when treatment is started early. However, if treatment is delayed, if the nerve damage is severe, or if follow-up care is missed, some degree of weakness, asymmetry, or facial tightness can remain permanently. Early consultation with a specialist gives you the best chance of complete recovery.
Q2. Can Bell’s palsy come back after it has healed?
Yes, it can — but it is uncommon. Roughly 7 to 15 percent of patients experience a recurrence, either on the same side or the opposite side. If Bell’s palsy returns on the same side more than once, this is a red flag. It should be investigated thoroughly with imaging, as recurring same-side palsy can sometimes indicate an underlying tumour or other structural cause rather than a simple nerve inflammation.
Final Thought
Bell’s palsy is common. It is often temporary. But it is never trivial — and it is never a condition to manage with guesswork.
The difference between full recovery, mild asymmetry, and lifelong facial tightness is often decided in the first 72 hours, and shaped by the quality of care and follow-up that follows. If you or someone you love is experiencing sudden facial weakness, do not delay.
Consult Dr. Akhilesh Kumar, trusted Neurosurgeon in Lucknow, for an accurate diagnosis, timely treatment, and a personalised recovery plan — because with Bell’s palsy, every hour counts.